The Creation of Movement: Foot to Ground Interaction
The Creation of Adam depicts the Biblical moment from Genesis when God gives life to the first man. It symbolises the spark of divine life - the connection between humanity and the holy.
Unfortunately for Michelangelo however, after spending four agonising years painting the ceiling of the Sistine Chapel 500 years ago, his most famous piece to me has come to represent the importance of feet (not fetishes), more so than the divine.
When thinking about human movement, it’s fundamentally created by the connection between two things: the foot and the ground. This is the physical touch point where forces generated by the body are imparted onto the floor, and transformed into locomotion. Something Stu McMillan, one of the most successful sprint coaches in the world, calls ‘foot to ground interaction’, and that I consider to be vitally important in any lower limb injury or neurological rehabilitation.
This was affirmed for on Tuesday during a session with one of my musculoskeletal clients who I’ve been rehabbing since September 2025 after she experienced 3 surgeries in 3 years following an ACL injury.
When she first came to me, she had participated in a significant amount of rehab, including with someone who was a mentor of mine and an industry leader in ACL recovery. Many had considered the knee, but few had considered Dan Pfaff’s question of “what else, where else?”, and during our initial assessment it became glaringly obvious to me that this client’s foot needed significant attention in any work we would do together. Let’s unpick why.
Firstly, from a principles level, your foot is how you interact with the ground, making it incredibly important for any task that requires you to traverse over that ground. Standing, walking, running, changing direction…they all require the foot to connect and interact with the floor, otherwise they don’t happen. Additionally, the brain also places a disproportionate weight on information flowing to and from the foot relative to the rest of the leg, illustrated by the humunculi below - depictions of how the body is represented in the somatosensory and motor cortices.
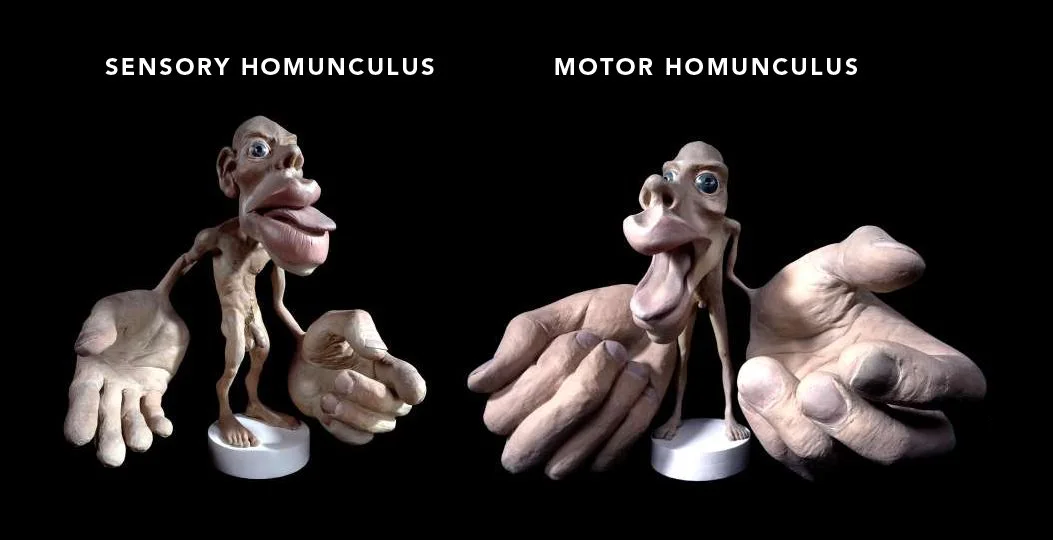
This makes the foot fundamentally important when considering anything to do with the human lower limb, particularly within the context of locomotion.
Secondly, during a simple movement assessment, this client’s feet - particularly the right foot on the previously injured limb - had mechanical properties more closely resembling that of a brick, as opposed to a marvel of evolutionary engineering containing 26 bones and 33 joints. The foot should be able to do many things, summarised by its two main dichotomous roles: to at times be a mobile adapter that changes shape and distributes force from the ground through the lower limb, and at others to be a rigid lever that freezes degrees of freedom and allows force to be transferred from the lower limb to the ground. This client’s left foot wasn’t doing either of these jobs very well, and her right foot wasn’t doing them at all.
Our final piece of the puzzle came during the mapping process using the Neubie device, where we took a low level of direct current electrical stimulation over various parts of the leg, simulating low level muscle contractions to assess how the nervous system responded. The idea being that if you artificially load a tissue using the Neubie that the brain has no problems with, the person continues to feel a consistent level of current. However, if you stimulate a tissue that the brain is protective of, this signal gets sent to the central nervous system, perceived as a threat, and leads to a low level pain response. It’s essentially the brain saying, “NOPE. Absolutely not. We’re not happy with that area being loaded and therefore we’re going to produce pain to warn you that you’re in danger.”, and if the brain isn’t happy with these spots, you can almost guarantee they’re not being used efficiently in day to day life.
We call these areas ‘hot spots’, and this client’s lower leg was littered with them. A minefield of arthrogenic muscle inhibition (AMI) laid by a brain limiting her capacity to use that leg again, terrified of any movement that might risk another injury. There were also plenty of hot spots within the hips and thighs, and over on the contralateral limb, but the highest concentration and subjectively most intense spots resided in the right shank.
So this was what we knew after this assessment: obviously the quads needed work, the hamstrings needed work, and the hips needed work, but the thread I wanted to emphasise in this dynamic fabric was the foot. So that’s what we did. Using targeted exercises and drills alongside the direct current of the Neubie device, we slowly convinced her brain that it didn’t need to be so protective of all of these hot spots. We did isolated work at the ankle, knee and hip to expand movement options, we did kinetic chain work that taught her how to use these options, and we did daily work on the foot that re-established the dialogue between the ground and her body.
The result has been no more day to day pain, no more pain in the gym, increased confidence, and a hope that she might be able to live her life unplagued by a stubborn knee that wouldn’t even let her crouch down or walk stairs without complaint. This isn’t all because of the work we’ve done down at the feet, but it’s formed the foundation of rebuilding a limb that can help her efficiently negotiate with the ground in ways that her nervous system now feels safe with, after 3 years and 3 surgeries (which are just traumatic injuries for your nervous system).
Just this week I was coaching her through a change of direction drill where our primary emphasis was on how the foot of her leg taking the penultimate step was interacting with the floor, allowing her to decelerate, redirect her force and transition to acceleration effectively. She was finding it challenging, as she should, but this is a skill that will allow her to share force across the entire lower limb, rather than leaving the knee vulnerable as has happened in the past.
As I said at the start of this blog, this concept isn’t just limited to musculoskeletal or injury rehab, but applies to anyone who wants to improve function in their lower limbs. In the session before the one described above, I was working on similar ideas with a client dealing with a neurodegenerative condition who first came to me wanting to improve her walking after a year of constant decline. We also placed a strong emphasis on improving both sensory and motor connection to the affected foot, and she’s now at a point where she can walk without using her ankle foot orthosis (AFO).
The moral of the story is - no matter your ailment, if you want to improve how you move and use your legs, it’s a great idea to start at the feet.